What is Rett Syndrome?
Rett syndrome is a severe neurological disorder that is diagnosed primarily in girls and begins to manifest during the toddler years. After a seemingly normal first year the child begins to regress with developmental milestones. This regression can happen quickly over a number of days or very gradually over months. Often the first noticeable symptoms include: low muscle tone (hypotonia), eye crossing, decreased interactions with people or surroundings, and loss of hand function. The hallmark symptom of Rett is repetitive hand movements and wringing that can be constant, especially in younger children.
As time passes additional symptoms may include: loss of speech, trouble with balance and motor coordination, irritability and crying, and disrupted sleep patterns. Many also develop seizures, anxiety, breathing problems, gastrointestinal issues, orthopedic complications, as well as oral motor difficulties.
It is important to note that Rett is a spectrum disorder, with children exhibiting a broad range of severity. Some individuals can say words of short phrases, can run, and feed themselves while others are unable to independently sit up. However, the symptoms in Rett are, unfortunately, oftentimes debilitating.

Our children are so much more than their symptoms. They are beautiful, they are powerful, and they are resilient. They inspire us to move mountains on their behalf.
Is there a Cure?
Although there currently is no cure for people with Rett syndrome, the sole focus of the Rett Syndrome Research Trust is to deliver cures as quickly as possible. We are optimistic because Rett-like symptoms are dramatically reversible in animal models of the disorder.
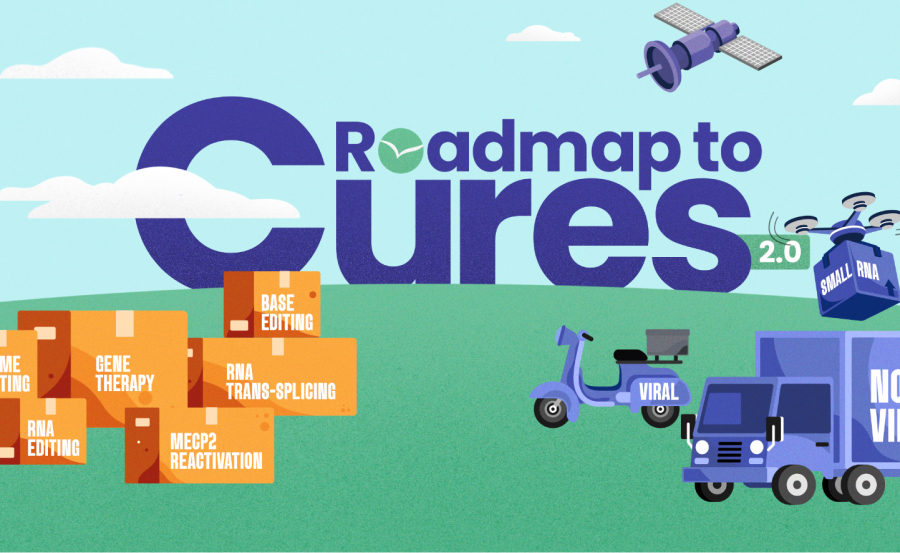
Curing the disorder requires targeting the root cause: mutations in the MECP2 gene. We are advancing genetic medicines that address Rett’s underlying cause and working aggressively to transition knowledge and resources to biopharmaceutical companies, which will further develop and commercialize a curative treatment.
Other Important Questions
Rett is caused by errors in a gene called MECP2, which is located on the X chromosome. All of us have an MECP2 gene in every one of our cells that makes a protein also called MECP2. Children with Rett have a mutation in the gene that causes the protein to not work properly. The MECP2 protein is present throughout the body, but it is especially important in the brain, where it helps keep brain cells functioning properly.
To better understand your child’s mutation and what it means for her future please visit our Genetics Primer.
Many studies have provided evidence that the vast majority of MECP2 mutations originate in the sperm. Since fathers give an X chromosome to their daughters and a Y chromosome to their sons, the MECP2 mutation in a sperm can only be transmitted from father to daughter. This is the reason why Rett is seen primarily in girls.
Due to the sheer volume of sperm that is continuously made it is likely that all men produce sperm with MECP2 mutations. One in about 20,000 eggs will be fertilized with a sperm that has an MECP2 mutation in it — the cruel reality of genetic roulette.
When boys have Rett their MECP2 mutation comes from their mother’s egg. Sometimes, however, the mutation can also originate in a single cell as the male embryo is developing. This is called somatic mosaicism.
Scientific papers over the years have hypothesized that because male fetuses have only one X chromosome their disease would be so severe that they might not develop to full term and the mothers might miscarry. However, there is no clinical data to support this hypothesis.

Rett syndrome is a clinical diagnosis given by a physician based on the child’s history and symptoms. An MECP2 mutation confirms a Rett diagnosis but is not required. In other words, it is possible to have a diagnosis of Rett without genetic confirmation or the other way around — an individual can have an MECP2 mutation without a clinical diagnosis of Rett syndrome.
If your child’s symptoms are consistent with Rett syndrome but your child has tested negative for an MECP2 mutation, please ensure that testing included sequencing all four exons of MECP2 and that deletion testing was done as well (sometimes called MLPA).

An individual with Rett will have a variety of problems that include loss of speech, loss of purposeful hand function, movement issues, seizures, gastrointestinal problems, orthopedic issues, autonomic issues, as well as sleep problems and anxiety.
Having compassionate doctors in place that will listen to you is key. In addition to a pediatrician, you may need a neurologist, a gastroenterologist, and an orthopedist. It’s important to note that not every child will have every symptom, so the team of doctors required to care for your child may vary.
Rett Healthcare Guidelines
Since most primary care doctors have limited experience with Rett syndrome, a consensus on guidelines about how to care for individuals with Rett syndrome was published in 2020. We hope this publication will be helpful to you, and we encourage you to share it with your child’s doctors.

Genetics 101
Mutations in a gene called MECP2 (methyl-CpG-binding protein 2) were identified as the cause of Rett syndrome in 1999, in the laboratory of Huda Zoghbi, MD, at Baylor College of Medicine. First discovered by Adrian Bird, PhD, in 1990, MECP2 produces a protein, also called MECP2, which regulates the activity of other genes. In most cases, the damaged copy of MECP2 can be traced to a random mutation in sperm. The incidence of recurrence in a family is less than 1%.
Although Rett syndrome remains a clinical diagnosis based on the child’s symptoms and history, the identification of MECP2 has made DNA testing and confirmation possible for affected individuals and their families. To date, approximately 95% of girls with a clinical diagnosis of Rett have a confirmed MECP2 mutation.
A History of Rett & RSRT

Andreas Rett publishes the first article on Rett syndrome in an obscure German medical journal which goes largely unnoticed.

Bengt Hagberg publishes the second article in a high-profile neurology journal and Rett gets noticed.
Adrian Bird publishes the discovery of the MECP2 protein. The first of many papers on MECP2.

After a 16 year search, Huda Zoghbi discovers that mutations in the MECP2 gene cause Rett.

Adrian Bird's lab discovers Rett symptoms in mice are reversible.

On the heels of Adrian Bird's reversal experiment, Monica launches the Rett Syndrome Research Trust with Adrian joining as a trustee.

MECP2 Consortium launched, a collaboration between Bird, Greenberg, and Mandel labs.

Gail Mandel and Brian Kaspar publish gene therapy results.

RSRT launches the MECP2 Gene Therapy Consortium.

RSRT launches $33 Million comprehensive research plan: Roadmap to a Cure.

Beam Therapeutics joins DNA editing effort.

CURE 360 launches — focused on driving forward the six genetic medicine strategies AND on business development.

Taysha Gene Therapies announces gene therapy program.

Vico Therapeutics announces RNA editing program.

Shape Therapeutics announces RNA editing program.

Alcyone Therapeutics announces their Rett program, ACTX-101, to reactivate the X chromosome.

Taysha Gene Therapies announces first gene replacement clinical trial.

Neurogene announces gene replacement program.

Taysha Gene Therapies doses patient #1 in gene replacement trial.
Neurogene doses first two patients.

Rett Syndrome Global Registry launches to help accelerate clinical trials.

MECP2 Editing Consortium launches to develop next-generation genetic medicines for Rett.
Roadmap to Cures 2.0 announced with goal of launching 3 new Clinical Trials by 2028.

RSRT gains access to a blood brain barrier penetrating capsid from Apertura Gene Therapy.
